Make Warfarin Dosing Safer & More Effective for your Patients
|
|
|
If you have patients who take warfarin, you know that achieving a stable INR can be a challenge. Too little warfarin leaves patients at risk for thrombosis. Too much can promote adverse bleeding events.
On average, 50% of major bleeding events associated with warfarin use occur in the first 90 days of treatment. Achieving a stable INR often requires trial and error with frequent and costly testing. The elevated risk of bleeding complications occurring in patients with unstable INRs often sways many physicians from prescribing warfarin to patients who could greatly benefit from it.
Today, with genetic testing, you have another tool to make warfarin dosing safer, less costly and more effective for your patients.
|
|
|
|
The Benefits of Testing: Optimal Dose, Fewer Adjustments, Faster Time to INR
Our Warfarin GenoSTAT Panel can help predict the optimal warfarin dose, may shorten the time to achieve stable dosing, reduce the need for dose adjustments, increase the time each patient spends in the target INR range, and has the potential to improve the overall safety and efficacy of warfarin therapy. Patients with some genetic variants are more likely to need lower doses of warfarin, take a longer time to reach target INR on starting therapy and may have an increased risk of bleeding complications.
Right Dosage? Look to Your Patient's Genes
There is a 10-fold inter-patient variability in the dosing required to attain a therapeutic response.2 Research has clearly shown that up to 40% of the individual variability in warfarin response can be accounted for by variations in two enzymes: CYP2C9 and VKORC1.3 CYP2C9 affects how warfarin is metabolized. VKORC1 affects how some patients respond to the drug.
|
|
|
|
A Closer Look at How Genotypes Affect Warfarin Metabolism
|
|
|
Warfarin is highly effective at antagonizing the vitamin K-dependent clotting pathway. Being a natural substance, it is given as a mixture of R and S stereoisomers (the chemical equivalent of mirror images). S-warfarin is three-to-five times more potent than its cousin, R-warfarin, in inhibiting the drug's target of action: the vitamin K epoxide reductase complex.
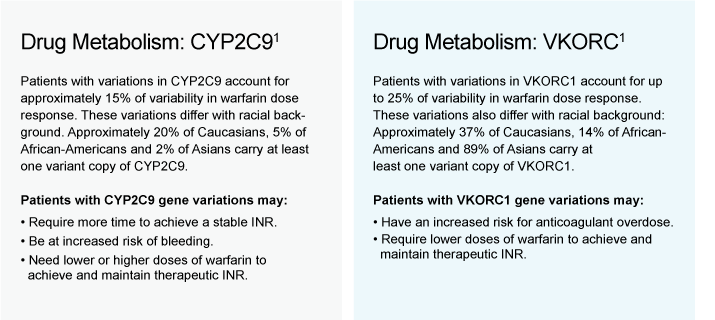
Phase I metabolism of S-warfarin is predominantly via the CYP2C9 enzyme. Genetic variations in this enzyme can affect the rate at which warfarin is inactivated and can play a major role in determining what an individual's maintenance dose of warfarin will be.
Patients with some genetic variants are more likely to need lower doses of warfarin, take a longer time to reach target INR on starting therapy and may have an increased risk of bleeding complications. The vitamin K epoxide reductase complex is responsible for converting vitamin K from an oxidized to a reduced state.
Reduced vitamin K is key to the formation of many of the proteins in the clotting cascade, and without it, overall coagulation is significantly inhibited. Warfarin inhibits the action of the major subunit of the vitamin K epoxide reductase complex: VKORC1. Variations in the VKORC1 subunit have been shown to be differentially sensitive to the action of warfarin.
Together, VKORC1 and CYP2C9 account for up to 40% of the individual variability in warfarin response. Other important variables include age, gender, height and weight, drug interactions and diet.3
|
|
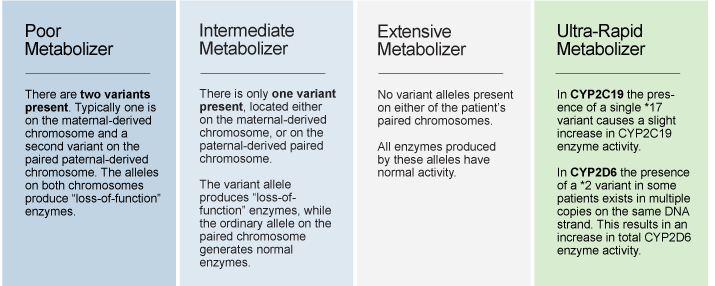
How Gene Variants Alter Enzyme Function, Drug Metabolism
|
|
|
|
Warfarin Genotyping Reduces Hospitalization Rates
|
|
|
In 2008, the FDA's Deputy Director of the Office of Clinical Pharmacology reported that:
"Prospective studies in different populations suggest that pharmocogenetic testing (for Warfarin) improves time to therapeutic INR and reduces adverse drug reactions."
These studies prompted the FDA to issue a Warfarin label change to alert physicians to the fact that Warfarin genotyping can significantly improve patient care. Additional prospective studies to measure the decrease in adverse bleeding and thrombosis have been underway. The first of these major prospective studies, the Mayo-Medco study, just reported its findings in the Journal of the American College of Cardiology.7
According to the Mayo-Medco study:
1. Genotyped patients had 31% fewer all-cause hospitalizations and 28% fewer hospitalizations for bleeding and thromboembolism.
2. Outcomes are improved: the earlier
the test results can be provided.
|
|
References
1. Andrew McWilliam, Randall Lutter, Clark Nardinelli. Health care savings from personalized medicine using genetic testing: the case of warfarin [Internet]. Working Paper 06-23, AEI-Brookings Joint Center for Regulatory Studies. 2006 [cited 2008 Nov 21]. Available from: http://aei-brookings.org/admin/authorpdfs/redirect-safely.php?fname=../pdffiles/WP06-23_topost.pdf
2. Fanikos J, Grasso-Correnti N, Shah R, Kucher N, Goldhaber SZ. Major bleeding complications in a specialized anticoagulation service. Am J Cardiol. 2005 Aug 15;96(4):595-598.
3. Bodin L, Verstuyft C, Tregouet DA, Robert A, Dubert L, Funck-Brentano C, Jaillon P, Beaune P, Laurent-Puig P, Becquemont L, et al. Cytochrome P450 2C9 (CYP2C9) and vitamin K epoxide reductase (VKORC1) genotypes as determinants of acenocoumarol sensitivity. Blood [Internet]. 2005 [cited 2008 Oct 24];106:135-140. Available from: http://bloodjournal.hematologylibrary.org/cgi/contne/full/106/1/135
4. FDA Approves Updated Warfarin (Coumadin) Prescribing Information [Internet]. U.S. Food and Drug Adminstration. 2007 [cited 2008 Oct 20]. Available from: http://www.fda.gov/bbs/topics/NEWS/2007/NEW01684.html
5. American Medical Association; Arizona CERT; Critical Path Institute. Personalized health care report 2008: warfarin and genetic testing [Internet]. 2008 [cited 2008 Nov 21]. Available at: http://www.azcert.org/medical-pros/warfarin_brochure.pdf
6. S.M. Huang, American Association of Clinical Chemisty annual meeting, July 2008
7. Robert S. Epstein et al., Warfarin Genotyping Reduces Hospitalization Rates: Results From the MM-WES (Medco-Mayo Warfarin Effectiveness Study) J. Am. Coll. Cardiol. 2010;55;2804-2812.
|
|
|
|
|
|
|
|
|
|
|
The AMA, the Critical Path Institute, and the Arizona Center for Education and Research on Therapeutics have collaborated to develop the brochure Personalized Health Care Report 2008: Warfarin and Genetic Testing. The brochure is designed for physicians and other health care providers who commonly prescribe warfarin but who may not have had exposure to pharmacogenomics and genetic testing.
|
|
The Warfarin GenoSTAT
tests specifically for
the following genes:
• CYP2C9
• VKORC1
|
|
|
|
|